基于标准集束化中心静脉导管干预策略观察儿科95万个导管日的每1000个导管日可减少3例导管相关血流感染发生的系统评价和Meta分析
摘要:目的 基于标准集束化中心静脉导管干预策略(简称标准集束化策略)对儿童中心静脉导管相关血流感染(CLABSI)文献进行系统评价和Meta分析,为预防和控制儿童CLABSI提供最佳证据体。方法 纳入同时符合以下标准的文献。①年龄<18岁的NICU和PICU住院患儿。②标准集束化策略:a.手卫生; b.置管过程中最大无菌屏障; c.浓度>0.5%的氯己啶、碘、碘伏作为皮肤消毒剂; d.每日评估导管的必要性,及时拔除不必要的导管; e.根据患儿特点选择最佳置管部位(非股静脉);至少满足上述5条中的前4条。③以1 000个导管日CLABSI发生事件数作为结局指标。④干预性研究的文献。;⑤文献语种不限。在Ovid-MEDLINE、Ovid-EMBASE、Web-of-science、Cochrane图书馆、中国生物医学文献数据库、中国知网、维普和万方数据库中进行检索,检索时间为2003年1月1日至2019年12月31日。采用ROBINS-I对纳入文献进行偏倚风险评价。结果 中英文数据库共检索到9 708篇文献,其他文献来源2篇,41篇文献进入本文分析,来自于20个国家,美国最多共18篇,均为历史对照研究。标准集束化策略为后时段干预措施,前时段干预措施不限。30篇研究场所为NICU,10篇研究场所为PICU,1篇研究场所为NICU和PICU。累计952 584个导管日,其中前时段干预措施442 296个导管日,后时段干预措施510 288个导管日。41篇文献中,低、中和高偏倚风险分别为11篇(27%)、18篇(44%)和12篇(29%)。标准集束化策略后可降低NICU+PICU患儿CLABSI发生事件数(I2=81%,随机效应模型),RR=0.40(95%CI:0.33~0.48),绝对效应值:每1 000个导管日可减少3(4~3)例CLABSI;可以降低NICU新生儿CLABSI发生事件数(I2=85%,随机效应模型),RR=0.36(95%CI:0.29~0.45);可以降低PICU患儿CLABSI发生事件数(I2=27%,固定效应模型),RR=0.54(95%CI:0.42~0.69)。结论 标准化集束化策略下每1 000个导管日可减少3~4例CLABSI。
关键词:集束化 中心静脉导管干预策略 儿科 中心静脉导管相关血流感染 导管日 Meta分析
中心静脉导管相关血流感染(CLABSI)是ICU院内感染监测的敏感指标,CLABSI不仅会导致住院费用的增加和住院时间的延长,甚至与患者的病死率有直接关系[1,2]。2011年美国危重症学会等16个学会或组织制定了《预防静脉导管相关性感染指南》[3],系统地强化了集束化中心静脉导管干预策略,指南中均以1 000个导管日CLABSI发生事件数作为结局指标。2014至2016年先后发表了主要以成人为研究对象的CLABSI的系统评价和Meta分析[4,5],2018年在BMJ上发表的系统评价和Meta分析[6]显示NICU集束化中心静脉导管干预策略可降低新生儿的CLABSI 60%。
本文基于标准集束化中心静脉导管干预策略(简称标准集束化策略),系统检索和评价文献,对NICU和PICU中CLABSI文献进行系统评价和Meta分析,期望为预防和控制儿科CLABSI提供当前最好证据体。
1 方法
1.1 集束化中心静脉导管干预策略
目前在儿科尚无公认的必须包括哪些项目才称之为集束化中心静脉导管干预策略,本文复习并综合文献[3,7-9],将以下5条作为集束化中心静脉导管干预策略的选项。(1)手卫生;(2)置管过程中最大无菌屏障;(3)浓度大于0.5%的氯己啶、碘、碘伏作为皮肤消毒剂;(4)每日评估导管的必要性,及时拔除不必要的导管;(5)根据患儿特点选择最佳置管部位(非股静脉)。本文以满足上述5条中的前4条即满足标准集束化策略,不排斥在5条之外的其他措施。
1.2 文献纳入标准
同时符合以下标准:(1)年龄<18岁的NICU和PICU住院患儿;(2)符合本文定义的标准集束化策略;(3)以1 000个导管日CLABSI发生事件数作为结局指标(1 000个导管日CLABSI发生事件数=CLABSI发生事件总数/导管总日数×1 000);(4)干预性研究的文献;(5)文献语种不限。
1.3 文献检索策略
1.3.1 检索数据库
英文数据库:Ovid-MEDLINE、OvidEMBASE、Web of Science、Cochrane图书馆临床对照试验资料库;中文数据库:中国生物医学文献数据库(CBM)、中国知网、维普、万方。
1.3.2 检索起止时间
2002年8月美国CDC发布的《预防静脉导管相关性感染指南》[7]比较系统地归纳了集束化中心静脉导管干预措施,且主要包含了本文1.1中的5项措施,故本文检索时间定于2003年1月1日至2019年12月31日。
1.3.3 英文文献检索
(1)检索词:intensive care,special care,critical*,nicu*,picu*,central,cv*,umbilic*,line*,picc,pcv,hickman,broviac,cvc*,clabsi*,catheter*,bundle*,program*,protocol*,checklist*,multidisiplin*,framework*,education*,quality*,improv*,prevent*,initiative*,manag*,hygiene*,hand washing,decontaminat*,disinfect。(2)检索式(以Web of Science为例):TS=((("intensive care"OR"special care"OR critical*OR icu OR nicu OR picu OR icus OR nicus OR picus))AND((((central OR cv OR cvp OR"subclavian vein"OR umbilic*)NEAR/3(catheter*OR line*))OR picc OR pcvl OR"cv cath"OR hickman OR broviac OR cvc OR cvcs OR"cla bsi"OR clabsi OR(catheter*NEAR/3("bloodstream infection"OR"bloodstream infections"OR bsi))))AND(((bundle*OR program*OR protocol*OR checklist*OR multidisciplin*OR framework*OR((education*OR qualit*OR improv*OR prevent*)NEAR/3(program*OR initiativ*OR collaborat*))OR (qualit*NEAR/3(manag*OR improv*))))OR(((hygien*OR"hand washing"OR decontaminat*ORdisinfect*ORnursing))AND((prevent*OR control*)))))。
1.3.4 中文文献检索
(1)检索词:中心静脉导管、集束化、集束化护理、集束化治疗、集束化干预、导管感染、导管相关性感染、导管相关性血流感染。(2)检索式:中心静脉导管AND(集束化OR集束化护理OR集束化治疗OR集束化干预)AND(导管感染OR导管相关性感染OR导管相关性血流感染)。
1.3.5 其他文献来源
阅读纳入文献的参考文献,筛选符合本文文献纳入标准的文献。
1.4 文献筛选原则
由康琼芳完成。通过阅读题目和摘要进行筛选,排除与中心静脉导管注入维护人相关、非干预类研究和纳入人群>18岁的文献;阅读全文进行再次筛选:(1)在中心静脉导管的护理干预措施中不能满足标准集束化策略5条中的前4条;(2)仅表述实施中心静脉导管的护理干预而无实质措施的描述,无法判定是否达到标准集束化策略;(3)不能从文献中提取或换算1 000个导管日CLABSI发生事件数;(4)干预人群包括成人和儿童,无法提取儿童数据的文献。
1.5 资料提取
由康琼芳提取,张崇凡和王瑞审核。文题、第一作者、发表年份、国家、研究的纳入和排除标准、研究场所、研究对象的基本特征、干预措施内容和实施过程、结局指标。主要结局指标:干预前、后中心静脉导管1 000个导管日CLABSI发生事件数;次要结局指标:标准集束化策略的依从性和经济学评价。
1.6 文献偏倚风险评价
由康琼芳评价。采用ROBINS-I(Risk Of Bias In Non-randomized Studies-of Intervention)[10]对纳入文献从混杂因素、受试对象选择、干预分类、修正/调整既定干预措施、数据缺失、结局测量、选择性报告7个维度行偏倚风险评价。若有不确定,与王瑞和张崇凡讨论决定。
1.7统计学方法
采用Revman 5.3软件完成提取数据的Meta整合,各效应量均以96%CI表示。对纳入的文献进行异质性检验,I2≤50时,采用固定效应模型合并;I2>50%,采用随机效应模型合并。计数资料采用作为统计分析的效应量。采用漏斗图法(Revman 5.3)检验发表偏倚。
2 结果
2.1 文献检索结果及特征
中、英文数据库共检索到9 706篇文献,其他文献来源2篇,经过筛选最终41篇文献进入本文分析,文献筛选流程见图1。
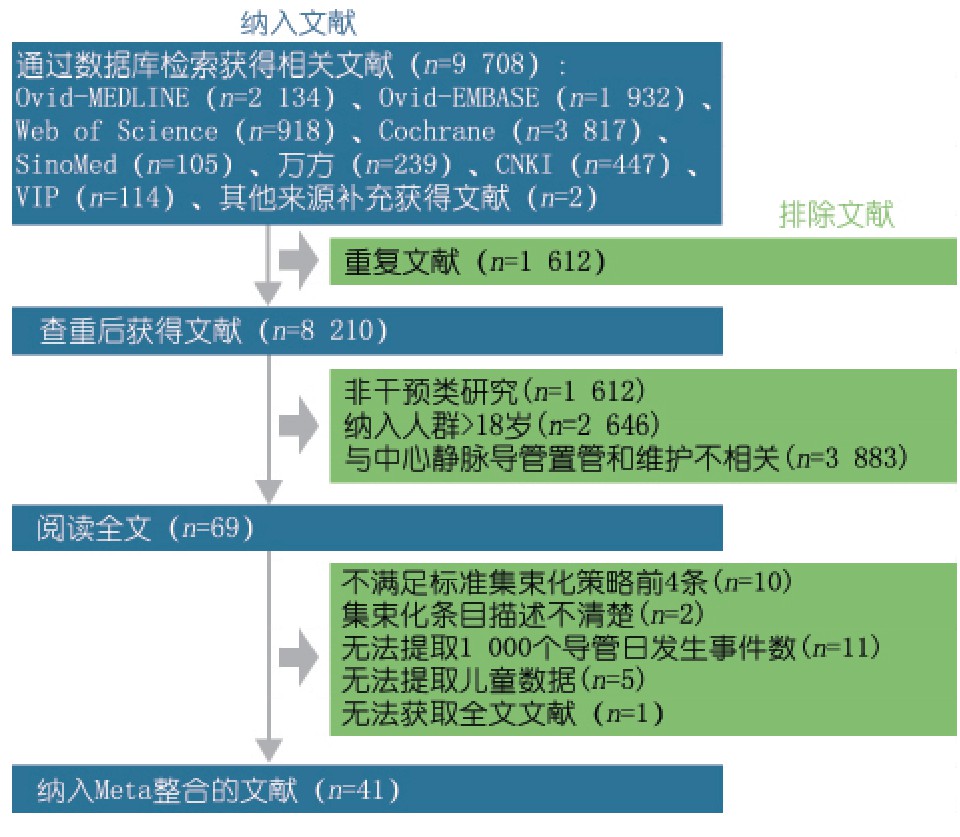
图1 文献纳入和排除流程图
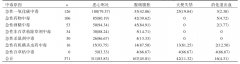
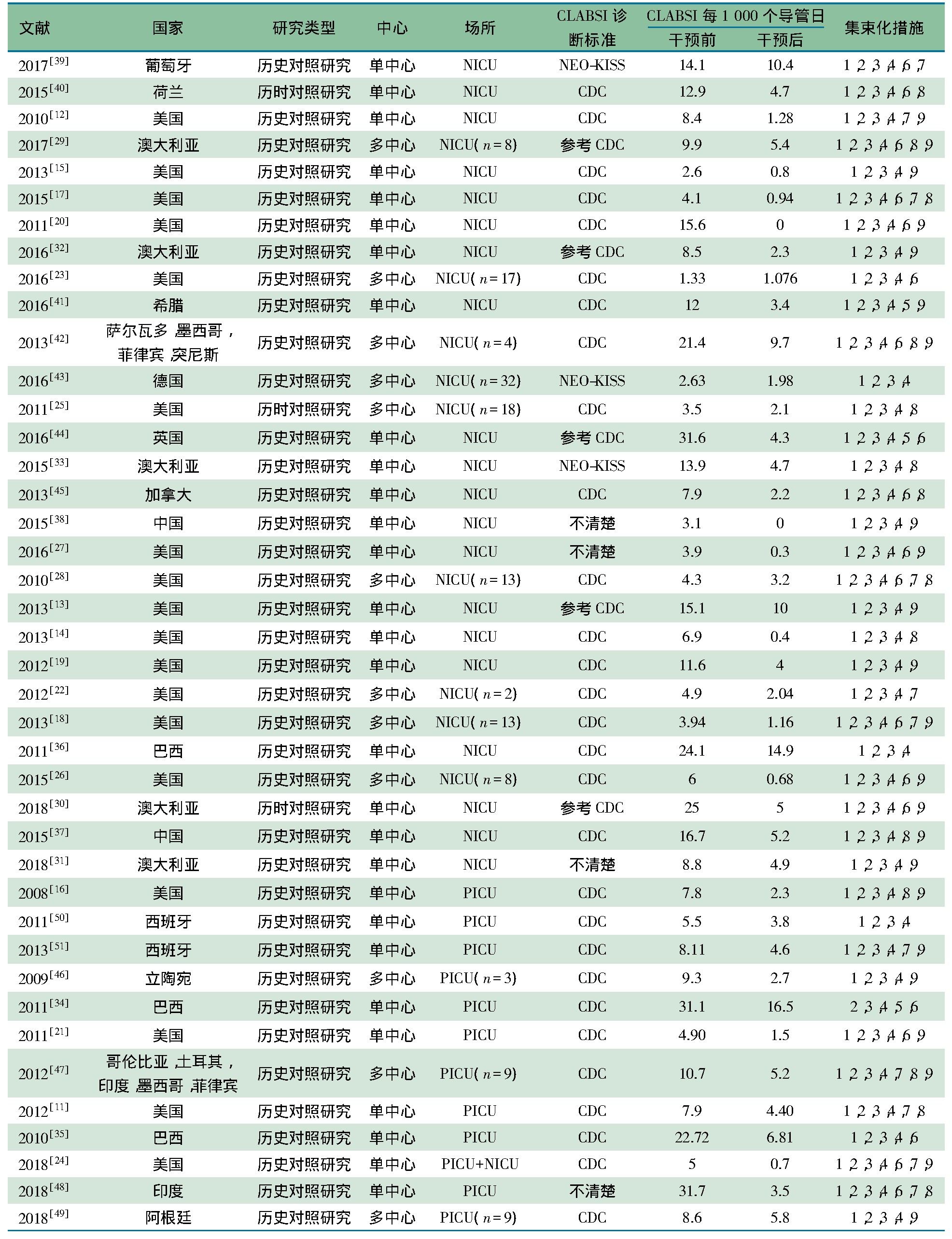
表1显示,41篇文献来自于20个国家,其中美国18篇[11-28],澳大利亚5篇[29-33],巴西3篇[50-51],西班牙[34-36]和中国[37,38]各2篇。均为历史对照研究。多中心研究12篇。研究场所:30篇为NICU,10篇为PICU,1篇[24]为NICU和PICU,共来自136个NICU和30个PICU。29篇采用CDC的CLABSI诊断标准,5篇[13,29,30,32,44]参考CDC的CLABSI诊断标准,3篇[33,39,43]采用新生儿科和ICU的早产儿医院感染监测系统(NEO-KISS)诊断标准,4篇[27,31,38,48]未具体说明CLABSI诊断标准。41篇文献累计952 584个导管日,其中前时段组442 296个导管日,后时段组510 288个导管日。满足本文标准集束化策略5条的有2篇文献[41,44],4条39篇,除5条之外的干预措施还包括导管接头的消毒、密闭式静脉通路、中心静脉工具箱、敷料的维护等。
表1 纳入文献的一般特征
 2.2文献偏倚风险评价
2.2文献偏倚风险评价
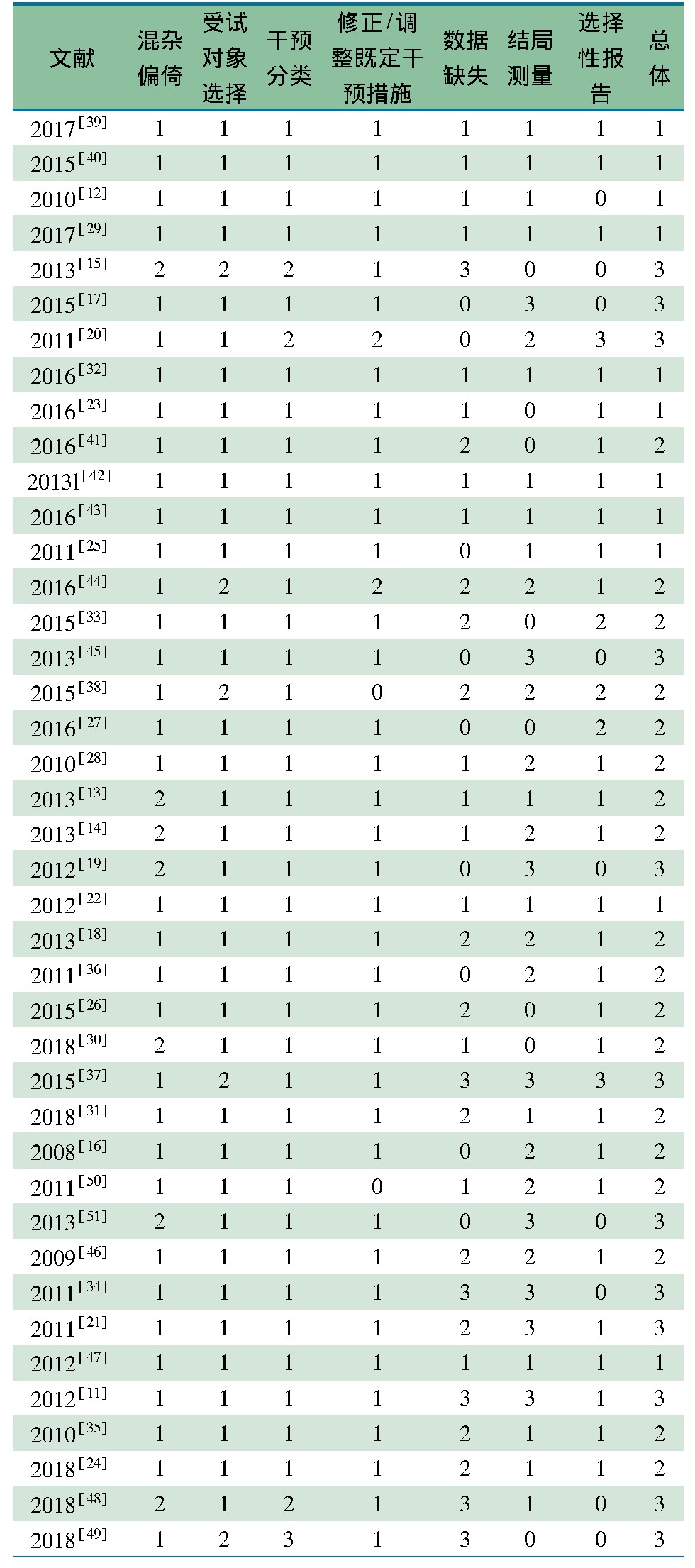
表2显示,纳入的41篇文献中,11篇(27%)低偏倚风险,18篇(29%)中偏倚风险,12篇(44%)高偏倚风险。41篇文献中,偏倚风险低34篇(83%),中7篇(17%);受试对象选择偏倚风险低36篇(88%),中5篇(12%);干预分类偏倚风险低37篇(90%),中3篇(7%),高1篇(3%);修正/调整既定干预措施偏倚风险低37篇(90%),中2篇(5%),不清楚2篇(5%);数据缺失偏倚风险低15篇(36%),中11篇(27%),高6篇(15%),不清楚9篇(22%);结局测量偏倚风险低15篇(36%),中10篇(24%),高8篇(20%),不清楚8篇(20%);选择性报告偏倚风险低27篇(66%),中3篇(7%),高2篇(5%),不清楚9篇(22%)。
表2 文献偏倚风险评价结果
 2.3 文献发表偏倚评价
2.3 文献发表偏倚评价
图2显示,(1)漏斗图总体对称;(2)右下角存在缺失,提示存在阴性结果数据有未发表的可能;(3)漏斗图数据集中在顶部,与以1 000个导管日为统计量计算感染发生事件有关。
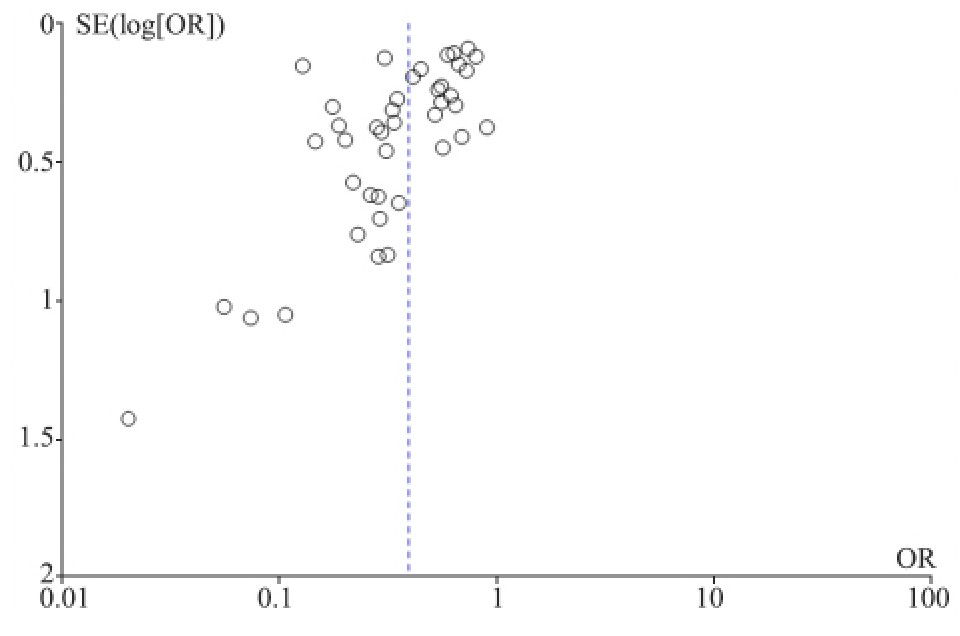 图2 集束化干预前后CLABSI发生事件的发表偏倚漏斗图
2.4 Meta分析
图2 集束化干预前后CLABSI发生事件的发表偏倚漏斗图
2.4 Meta分析
2.4.1 主要结局指标
基于标准集束化策略对31篇以PICU为干预场所和11篇以NICU为干预场所患儿CLABSI发生事件进行了汇总。图3显示,I2=81%,随机效应模型合并,标准集束化策略后可以降低NICU+PICU患儿CLABSI发生事件数,RR=0.40(95%CI:0.33~0.48),差异有统计学意义(P<0.000 01);绝对效应值为每1 000个导管日可减少3(4~3)例CLABSI。
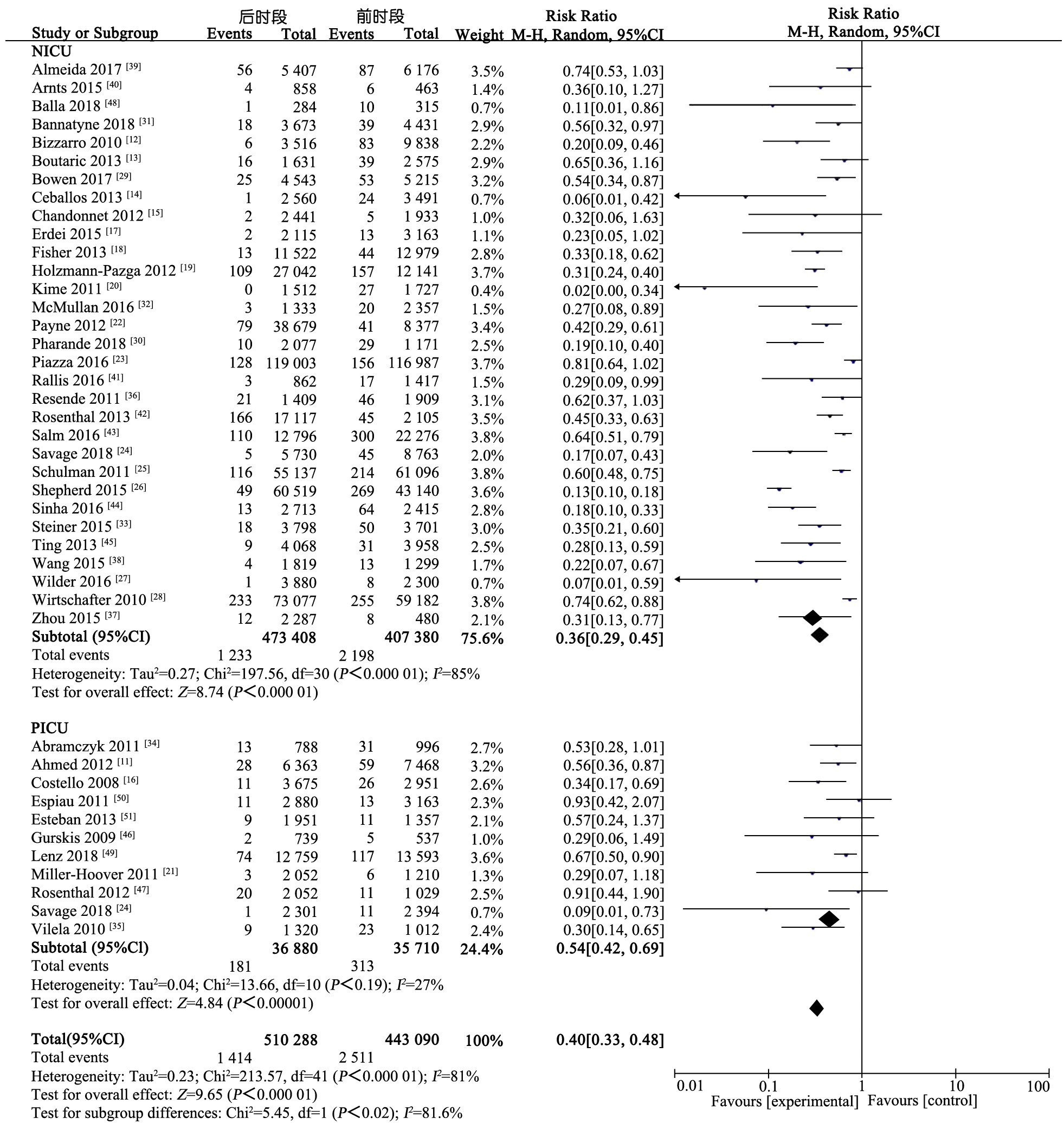 图3 标准集束化干预对中心静脉导管CLABSI发生事件的Meta分析
NICU干预场所的亚组分析,I2=85%,随机效应模型合并,标准集束化策略后可降低新生儿CLABSI发生事件数,OR=0.36(95%CI:0.29~0.45),差异有统计学意义(P<0.000 01);绝对效应值为每1 000个导管日可减少3(4~3)例CLABSI。PICU干预场所的亚组分析,I2=27%,固定效应模型合并,标准集束化策略可降低PICU患儿的CLABSI发生事件数,OR=0.54(95%CI:0.42~0.69),差异有统计学意义(P<0.001);绝对效应值为每1 000个导管日可减少4(5~3)例CLABSI。
图3 标准集束化干预对中心静脉导管CLABSI发生事件的Meta分析
NICU干预场所的亚组分析,I2=85%,随机效应模型合并,标准集束化策略后可降低新生儿CLABSI发生事件数,OR=0.36(95%CI:0.29~0.45),差异有统计学意义(P<0.000 01);绝对效应值为每1 000个导管日可减少3(4~3)例CLABSI。PICU干预场所的亚组分析,I2=27%,固定效应模型合并,标准集束化策略可降低PICU患儿的CLABSI发生事件数,OR=0.54(95%CI:0.42~0.69),差异有统计学意义(P<0.001);绝对效应值为每1 000个导管日可减少4(5~3)例CLABSI。
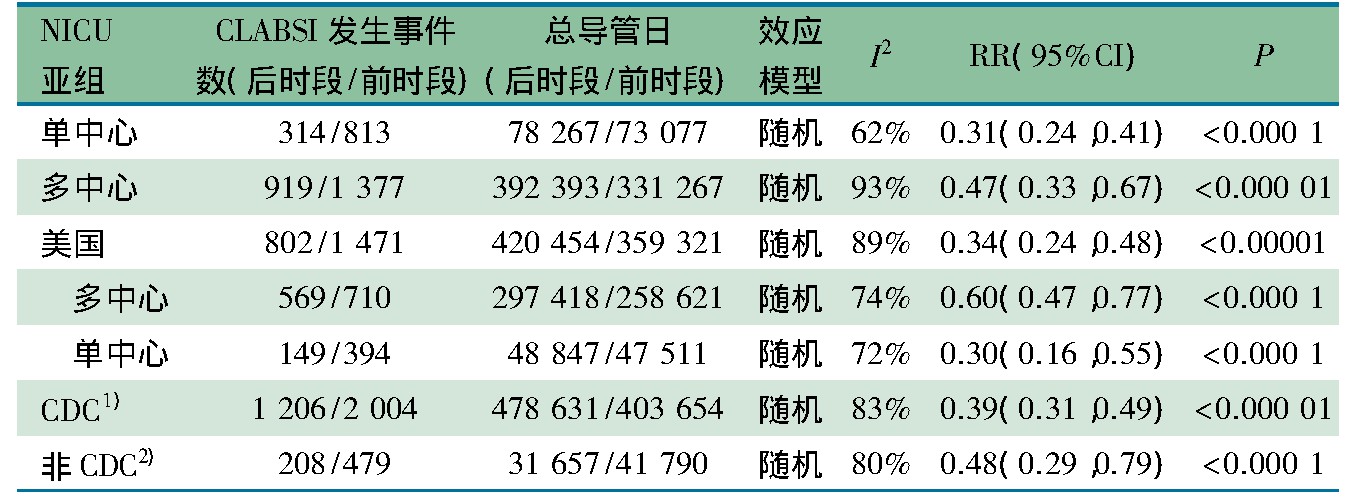
标准集束化策略对中心静脉导管CLABSI发生事件的Meta分析存在较大异质性(I2=81%),造成异质性的来源考虑:(1)NICU干预场所的亚组的异质性(I2=85%),鉴于83.9%(26/31)的文献无法提取临床异质性的因素(如胎龄、出生体重、疾病严重程度、置管部位、导管种类等),故以单中心和多中心角度、最多文献报道国家角度(31篇以NICU干预场所的亚组文献中美国占42%,其中多中心5篇、单中心8篇)分析异质性来源。表3显示,单中心研究RR=0.31(95%CI:0.24~0.41),I2=62%;多中心研究RR=0.47(95%CI:0.33~0.67),I2=93%;美国以NICU干预场所的标准集束化策略对中心静脉导管CLABSI发生事件,RR=0.34(95%CI:0.24~0.48),I2=89%;美国单中心研究RR=0.60(0.47~0.77),I2=74%;美国多中心研究RR=0.30(0.16,0.55),I2=74%。(2)CLABSI诊断标准,表3显示,采用和参考了CDC的CLABSI诊断标准的患儿标准集束化策略对中心静脉导管CLABSI发生事件,RR=0.39(95%CI:0.31~0.49),I2=83%。采用NEO-KISS标准+未具体说明诊断标准的患儿标准集束化策略对CLABSI发生事件,RR=0.48(95%CI:0.29~0.79),I2=80%。
表3 亚组分析可能异质性来源
 2.4.2 次要结局指标
2.4.2 次要结局指标
2.4.2. 1 对标准集束化策略的依从性
从41篇文献提取本文标准集束化策略项目,仅提取到手卫生[16,17]和最大无菌屏障[21]依从性结局,手卫生从干预前38%~73%提升到干预后85.5%~100%,最大无菌屏障从干预前85%提升到干预后100%。
2.4.2. 2 对标准集束化策略经济学评价
41篇文献中仅有2篇文献涉及了经济学评价。Ahmed等[11]发现,通过24个月的标准集束化策略,避免了50例CLABSI的发生,6例潜在死亡,基于每次29 000美元CLABSI治疗,相当于节约了145万美元;Ceballos等[14]通过以护士为主导的质量改进项目(符合标准集束化策略的前4项)减少了84 d的住院日,估计节省了34.8万美元成本。
3 讨论
本文纳入的41篇文献来自于20个国家,主要集中在发达国家,其中美国最多(18篇);2002年8月美国CDC发布《预防静脉导管相关性感染指南》[7],指南中比较系统地归纳了集束化中心静脉导管干预措施,本文检索时间2003年初至2019年底,2008至2010年5篇,2011至2015年23篇,2016至2018年13篇,相关文献发表时限表明,集束化中心静脉导管干预是晚近10年预防CLABSI的关注热点;41篇文献中多中心研究虽然仅占29%(12篇),但总导管日占73%(693 660/952 584),CLABSI发生事件数占67%(2 296/3 423);文献发表偏倚漏斗图总体对称,尽管漏斗图右下角存在缺失,但处于底部样本量不大,不会对结果造成影响;41篇文献偏倚风险评估中,29%(12篇)为高偏倚风险并且均为单中心研究,27%(11篇)为低偏倚风险,其中64%(7/11)为多中心研究。本文系统评价和Meta分析基于标准集束化策略观察的95万个导管日的每1 000个导管日CLABSI发生事件数的结果是有信心的。
2011年CDC发布的以成人和儿童为应用对象的《中心静脉导管相关感染预防指南》[3],首次将集束化的中心静脉管理策略推荐为该领域质量控制和质量改进的方法,该策略在儿科应用效果尚不清楚。本研究通过对CLABSI预防指南[3,7-9]的文献回顾,形成适合儿科基于标准集束化策略,其中前4条均具有较好的推广性,在任何水平的NICU和PICU均是应知应会的项目。第5条“根据患儿特点选择最佳置管部位(非股静脉)”,在儿科文献报告中较少将其纳入集束化策略项目中,可能因置管部位的选择与置管医生的能力、资质更相关[52],尽管如此,本文仍然认为置管部位的选择是集束化策略中不可忽视的重要方面,应当作为标准集束化策略的项目,鉴于本文纳入的儿科文献中较少体现第5条,故本研究提出的标准集束化策略应至少满足前4条。
对CLABSI的结局指标存在不同的定义,既往以中心静脉置管总病例数中CLABSI发生例数为结局指标[53,54],这种结局统计方法的缺陷在于忽视了导管留置时间与CLABSI发生率的相关性。目前国际上公认的是,以1 000个导管日CLABSI的发生数作为结局指标,其优点在于既能体现中心静脉置管CLABSI发生率,也能体现导管留置时间与CLABSI发生率的正相关性。本文采用每1 000个导管日CLABSI的发生率为效应量进行Meta分析,以中心静脉置管总病例数中CLABSI发生例数为结局指标的文献,只要文献中给出CLABSI发生率的频数比和导管留置总天数,本文都可换算为每1 000个导管日CLABSI的发生率。
本文CLABSI发生事件数观察样本达到95万个导管日,是当前相关研究最大样本量的系统评价和Meta分析,标准集束化策略可降低NICU+PICU患儿CLABSI发生事件。可降低NICU和PICU患儿CLABSI发生事件60%和46%。标准集束化策略后,不论是在NICU,还是在PICU,还是NICU+PICU,每1 000个导管日可减少3~4例CLABSI的结果均有信心,不仅体现在相对RR值,而且体现在绝对效应值。
本文标准集束化策略对中心静脉导管CLABSI发生事件的Meta分析提示存在较大异质性(I2=81%),尽管本文从NICU干预场所的亚组角度、多中心与单中心角度、最多研究文献国家角度、是否采用CDC的CLABSI诊断标准角度考察了异质性的来源,但均没有得到异质性确切来源,造成异质性的来源可能为临床异质性,特别是NICU临床异质性,NICU的CLABSI发生事件与胎龄、出生体重、疾病严重程度、置管部位、导管种类密不可分,但纳入文献均忽视相关描述。
参考文献
[1]Ziegler MJ,Pellegrini DC,Safdar N. Attributable mortality of central line associated bloodstream infection:systematic review and meta-analysis. Infection,2015,43(1):29-36.
[2]Stevens V,Geiger K,Concannon C,et al. Inpatient costs,mortality and 30-day re-admission in patients with central-lineassociated bloodstream infections. Clin Microbiol Infect,2014,20(5):318-324.
[3]O'grady NP,Alexander M,Burns LA,et al. Guidelines for the prevention of intravascular catheter-related infections. Am J Infect Control,2011,39(4 Suppl 1):S1-34.
[4]Blot K,Bergs J,Vogelaers D,et al. Prevention of central line-associated bloodstream infections through quality improvement interventions:a systematic review and metaanalysis. Clin Infect Dis,2014,59(1):96-105.
[5]Ista E,Van Der Hoven B,Kornelisse RF,et al. Effectiveness of insertion and maintenance bundles to prevent central-lineassociated bloodstream infections in critically ill patients of all ages:a systematic review and meta-analysis. Lancet Infect Dis,2016,16(6):724-734.
[6]Payne V,Hall M,Prieto J,et al. Care bundles to reduce central line-associated bloodstream infections in the neonatal unit:a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed,2018,103(5):F422-F429.
[7]O'grady NP,Alexander M,Dellinger EP,et al. Guidelines for the prevention of intravascular catheter-related infections. Am J Infect Control,2002,30(8):476-489.
[8]Jalil BA,Cavallazzi R. Predicting fluid responsiveness:A review of literature and a guide for the clinician. Am J Emerg Med,2018,36(11):2093-2102.
[9]Gorski LA. The 2016 Infusion Therapy Standards of Practice.Home Healthc Now,2017,35(1):10-18.
[10]Sterne JA,Hernan MA,Reeves BC,et al. ROBINS-I:a tool for assessing risk of bias in non-randomised studies of interventions. Bmj,2016,355:i4919.
[11]Ahmed SS,Mccaskey MS,Bringman S,et al. Catheterassociated bloodstream infection in the pediatric intensive care unit:a multidisciplinary approach. Pediatr Crit Care Med,2012,13(2):e69-72.
[12]Bizzarro MJ,Sabo B,Noonan M,et al. A quality improvement initiative to reduce central line-associated bloodstream infections in a neonatal intensive care unit. Infect Control Hosp Epidemiol,2010,31(3):241-248.
[13]Boutaric E,Gilardi M,Cécile W,et al. Impact of clinical practice guidelines on the incidence of bloodstream infections related to peripherally inserted central venous catheter in preterm infants. Arch Pediatr,2013,20(2):130-136.
[14]Ceballos K,Waterman K,Hulett T,et al. Nurse-driven quality improvement interventions to reduce hospital-acquired infection in the NICU. Adv Neonatal Care,2013,13(3):154-163,quiz 164-165.
[15]Chandonnet CJ,Kahlon PS,Rachh P,et al. Health care failure mode and effect analysis to reduce NICU line-associated bloodstream infections. Pediatrics,2013,131(6):e1961-1969.
[16]Costello JM,Morrow DF,Graham DA,et al. Systematic intervention to reduce central line-associated bloodstream infection rates in a pediatric cardiac intensive care unit.Pediatrics,2008,121(5):915-923.
[17]Erdei C,Mcavoy LL,Gupta M,et al. Is zero central lineassociated bloodstream infection rate sustainable? A 5-year perspective. Pediatrics,2015,135(6):e1485-1493.
[18]Fisher D,Cochran KM,Provost LP,et al. Reducing central line-associated bloodstream infections in North Carolina NICUs.Pediatrics,2013,132(6):e1664-1671.
[19]Holzmann-Pazgal G,Kubanda A,Davis K,et al. Utilizing a line maintenance team to reduce central-line-associated bloodstream infections in a neonatal intensive care unit. J Perinatol,2012,32(4):281-286.
[20]Kime T,Mohsini K,Nwankwo MU,et al. Central line"attention"is their best prevention. Adv Neonatal Care,2011,11(4):242-8,quiz 249-250.
[21]Miller-Hoover S. Pediatric central line:bundle implementation and outcomes. J Infus Nurs,2011,34(1):36-48.
[22]Payne NR,Barry J,Berg W,et al. Sustained reduction in neonatal nosocomial infections through quality improvement efforts. Pediatrics,2012,129(1):e165-173.
[23]Piazza AJ,Brozanski B,Provost L,et al. SLUG Bug:Quality Improvement With Orchestrated Testing Leads to NICU CLABSI Reduction. Pediatrics,2016,137(1). doi:10. 1542/peds.
[24]Savage T,Hodge DE,Pickard K,et al. Sustained reduction and prevention of neonatal and pediatric central line-associated bloodstream infection following a nurse-driven quality improvement initiative in a pediatric facility. JAVA,2018,23(1):30-41.
[25]Schulman J,Stricof R,Stevens TP,et al. Statewide NICU central-line-associated bloodstream infection rates decline after bundles and checklists. Pediatrics,2011,127(3):436-444.
[26]Shepherd EG,Kelly TJ,Vinsel JA,et al. Significant reduction of central-line associated bloodstream infections in a network of diverse neonatal nurseries. J Pediatr,2015,167(1):41-46.e1-3.
[27]Wilder KA,Wall B,Haggard D,et al. CLABSI reduction strategy:A systematic central line quality improvement initiative integrating line-rounding principles and a team approach. Adv Neonatal Care,2016,16(3):170-177.
[28]Wirtschafter DD,Pettit J,Kurtin P,et al. A statewide quality improvement collaborative to reduce neonatal central lineassociated blood stream infections. J Perinatol,2010,30(3):170-81.
[29]Bowen JR,Callander I,Richards R,et al. Decreasing infection in neonatal intensive care units through quality improvement. Arch Dis Child Fetal Neonatal Ed,2017,102(1):F51-F57.
[30]Pharande P,Lindrea KB,Smyth J,et al. Trends in late-onset sepsis in a neonatal intensive care unit following implementation of infection control bundle:A 15-year audit.Journal of Paediatrics and Child Health,2018,54(12):1314-1320.
[31]Bannatyne M,Smith J,Panda M,et al. Retrospective cohort analysis of central line associated blood stream infection following introduction of a central line bundle in a neonatal intensive care unit. Int J Pediatr,2018:4658181.
[32]Mcmullan R,Gordon A. Impact of a central line infection prevention bundle in newborn infants. Infect Control Hosp Epidemiol,2016,37(9):1029-1036.
[33]Steiner M,Langgartner M,Cardona F,et al. Significant reduction of catheter-associated blood stream infections in preterm neonates after implementation of a care bundle focusing on simulation training of central line insertion. Pediatr Infect Dis J,2015,34(11):1193-1196.
[34]Abramczyk ML,Carvalho WB,Medeiros EA. Preventing catheter-associated infections in the Pediatric Intensive Care Unit:impact of an educational program surveying policies for insertion and care of central venous catheters in a Brazilian teaching hospital. Braz J Infect Dis,2011,15(6):573-577.
[35]Vilela R,Dantas SRPE,Trabasso P. Interdisciplinary taskforce reduces catheter-related bloodstream infection in a Pediatric Intensive Care Unit. Rev Paul Pediatr,2010,28(4):292-298.
[36]Resende DS,OJM,BritoD,et al. Reduction of catheterassociated bloodstream infections through procedures in newborn babies admitted in a university hospital intensive care unit in Brazil. Rev Soc Bras Med Trop,2011,44(6):731-734.
[37]Zhou Q,Lee SK,Hu XJ,et al. Successful reduction in central line-associated bloodstream infections in a Chinese neonatal intensive care unit. Am J Infect Control,2015,43(3):275-279.
[38]Wang W,Zhao C,Ji Q,et al. Prevention of peripherally inserted central line-associated blood stream infections in very low-birth-weight infants by using a central line bundle guideline with a standard checklist:a case control study. BMC Pediatr,2015,15:69.
[39]Almeida CC,Pissarra Da Silva SMS,Flor De Lima Caldas De Oliveira FSD,et al. Nosocomial sepsis:evaluation of the efficacy of preventive measures in a level-III neonatal intensive care unit. J Matern Fetal Neonatal Med,2017,30(17):2036-2041.
[40]Arnts IJ,Schrijvers NM,Van Der Flier M,et al. Central line bloodstream infections can be reduced in newborn infants using the modified Seldinger technique and care bundles of preventative measures. Acta Paediatr,2015,104(4):e152-157.
[41]Rallis D,Karagianni P,Papakotoula I,et al. Significant reduction of central line-associated bloodstream infection rates in a tertiary neonatal unit. Am J Infect Control,2016,44(4):485-487.
[42]Rosenthal VD,Dueas L,Sobreyra-Oropeza M,et al.Findings of the International Nosocomial Infection Control Consortium(INICC),part III:effectiveness of a multidimensional infection control approach to reduce central line-associated bloodstream infections in the neonatal intensive care units of 4 developing countries. Infect Control Hosp Epidemiol,2013,34(3):229-237.
[43]Salm F,Schwab F,Geffers C,et al. The implementation of an evidence-based bundle for bloodstream infections in neonatal intensive care units in germany:A controlled intervention study to improve patient safety. Infect Control Hosp Epidemiol,2016,37(7):798-804.
[44]Sinha AK,Murthy V,Nath P,et al. Prevention of Late Onset Sepsis and Central-line Associated Blood Stream Infection in Preterm Infants. Pediatr Infect Dis J,2016,35(4):401-406.
[45]Ting JY,Goh VS,Osiovich H. Reduction of central lineassociated bloodstream infection rates in a neonatal intensive care unit after implementation of a multidisciplinary evidencebased quality improvement collaborative:A four-year surveillance. Can J Infect Dis Med Microbiol,2013,24(4):185-190.
[46]Gurskis V,Asembergiene J,Kevalas R,et al. Reduction of nosocomial infections and mortality attributable to nosocomial infections in pediatric intensive care units in Lithuania.Medicina(Kaunas),2009,45(3):203-213.
[47]Rosenthal VD,Ramachandran B,Villamil-Gómez W,et al.Impact of a multidimensional infection control strategy on central line-associated bloodstream infection rates in pediatric intensive care units of five developing countries:findings of the International Nosocomial Infection Control Consortium(INICC). Infection,2012,40(4):415-423.
[48]Balla KC,Rao SPN,Arul C,et al. Decreasing Central Lineassociated Bloodstream Infections Through Quality Improvement Initiative. Indian Pediatr. 2018,55(9):753-756.
[49]Lenz AM,Andion E,Ruvinsky S,et al. Impact of a program aimed at reducing catheter-related infections implemented in nine pediatric intensive care units in Argentina. Arch Argent Pediatr,2018,116(2):93-97.
[50]Espiau M,Pujol M,Campins-MartíM,et al. Incidence of central line-associated bloodstream infection in an intensive care unit. An Pediatr(Barc),2011,75(3):188-193.
[51]Esteban E,Ferrer R,Urrea M,et al. The impact of a quality improvement intervention to reduce nosocomial infections in a PICU. Pediatr Crit Care Med,2013,14(5):525-532.
[52]Cameron KA,Cohen ER,Hertz JR,et al. Barriers and facilitators to central venous catheter insertion:A qualitative study. J Patient Saf,2018. doi:10. 1097/PTS.0000000000000477.
[53]吕会玲,程丽楠.国内集束化护理预防深静脉导管相关性血流感染效果的Meta分析.中国实用护理杂志,2014,30(31):69-72.
[54]郑艳,吴君,李莉,等.中心静脉集束化干预策略预防导管相关性血流感染的Meta分析.护理学报,2016,23(8):56-60.